

Introduction: Bruton tyrosine kinase (BTK) inhibitors are a class of drugs that inhibit B-cell receptor (BCR) and are increasingly used in B-cell lymphoproliferative neoplasms, including chronic lymphocytic leukemia (CLL), mantle cell lymphoma (MCL), and Waldenstrom's macroglobulinemia. Ibrutinib, a first-generation BTK inhibitor has been associated with increased risk of cardiovascular adverse events (AEs), including atrial fibrillation (AF), hypertension (HTN) and bleeding. These unique AEs are thought to be due to off-target effects. Acalabrutinib, a second-generation BTK inhibitor is characterized by less off-target effects, and is thought to be associated with a decreased risk of cardiovascular and other AEs. However, a head to head comparison of ibrutinib and acalabrutinib has not been conducted. Herein, we conducted a systematic review and network meta-analysis of AEs from prospective clinical trials of ibrutinib and acalabrutinib in B-cell lymphoproliferative disorders to compare their safety profile.
Methods: We searched PubMed, Embase, Scopus, and Web of Science from database inception through November 15th 2019. Only full-text articles were included. Other inclusion criteria included prospective trials (single arm or randomized) with ibrutinib, ibrutinib plus anti-CD20 antibody, or acalabrutinib as investigational agents. Trials investigating BTK inhibitor plus chemotherapy were excluded. When updated results of prospective trials were available, data were extracted from the most recent publication with the longest follow-up. Reports of 17 AEs of interest, including number of events (any grade and grade 3 or higher) were documented. Rate of discontinuation was investigated.
Results: Twenty-seven prospective clinical trials, 12 multicenter single-arm, 9 multicenter randomized, 5 single center single-arm, and 1 single center randomized, were included. Data from 29 study arms including 3207 patients were analyzed in 3 groups - ibrutinib, ibrutinib plus anti-CD20 antibody, and acalabrutinib with augmented Bayesian network meta-analysis and meta-regression implemented in R including packages gemtc and rjags. The most common any grade AEs (>20%) with ibrutinib were diarrhea (46%, 95% CI 36-55%), myalgias/arthralgias (37%, 95%CI 28-46%), fatigue (33%, 95% CI 24-42%), cough (26%, 95% 17-36%), anemia (23%, 95% 15-30%), thrombocytopenia (22%, 95% 15-30%), and pyrexia (21%, 95% 13-30%). The most common any grade AEs with acalabrutinib were headache (37%, 95%CI 26-48%), diarrhea (30%, 95% 20-41%), peripheral edema (21%, 95% 15-28%), fatigue (20%, 95% 11-29%), and myalgias/arthralgias (16%, 95% 8-24%). The most common any grade cardiovascular AEs with ibrutinib were bleeding/bruising (32%, 95% 23-41%), HTN (23%, 95% 15-32%), AF (9%, 95% 3-15%). The most common any grade cardiovascular AEs with acalabrutinib were bleeding/bruising (41%, 95% CI 30-52%), and HTN (6%, 95% 1-11%).
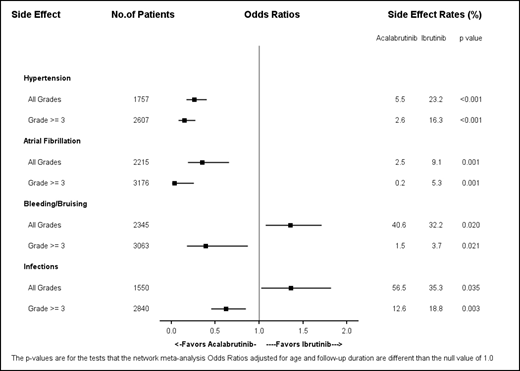
The rate of AEs with ibrutinib compared to ibrutinib plus anti-CD20 antibody were similar so the data was pooled. Of all AEs of interest, there was a significant difference in any grade AEs favoring ibrutinib for headache (12% vs. 37%), and infections (35% vs 57%). There was a significant difference in any grade AEs favoring acalabrutinib for myalgias/arthralgias (16% vs. 37%), anemia (6% vs. 23%), thrombocytopenia (5% vs. 22%), and HTN (6% vs. 23%). After adjusting for median follow-up and age, there was no significant difference in rates of bleeding/bruising and any grade infections between ibrutinib and acalabrutinib. However, there was a significant difference favoring acalabrutinib for any grade HTN (OR 0.26, 95% CI 0.17-0.40) p<0.0001, grade 3 HTN (OR 0.15, 95% 0.08-0.27) p<0.0001, any grade AF (OR 0.35, 95% 0.18-0.66), p=0.0012, grade 3 AF (OR 0.04, 95% 0.01-0.25) p=0.0009, and grade 3 infections (OR 0.62, 95% 0.46-0.85),p=0.003.
Conclusions: Acalabrutinib appears to have an overall improved safety profile compared to ibrutinib. This is particularly true for anemia, thrombocytopenia, and cardiovascular AEs, including AF and HTN.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal